Mucosal Melanoma of the Head & Neck
- Mucosal melanomas are rare (<1% of all melanomas), but are very aggressive and have features that are distinct from cutaneous melanoma
- Around 55% of all mucosal melanomas arise within the head and neck region.
- 2/3 of these arise within the nasal cavity or paranasal sinuses
- 1/4 arise within the oral cavity
- The remainder occur sporadically in other sites within the head and neck.
- Historically, the Ballantyne staging system (1970) was used to classify mucosal melanoma across all sites including outside of the head and neck.
- The Ballantyne staging system simply classified tumours as Stage I (confined to the primary site), Stage II (regional lymph node involvement), or Stage III (distal metastasis).
- Mucosal melanomas involving the nasal cavity or paranasal sinuses were also previously staged with the AJCC system for nasal cavity and paranasal sinus carcinoma.
- However, evidence suggested that this did not discriminate prognosis between stages with mucosal melanoma well.
- This also did not provide a staging system for MMs of the other potential disease sites in the head and neck.
- This prompted the creation of a separate staging system for mucosal melanoma involving the head and neck, which was introduced in the AJCC 7th Edition, and remains unchanged in the 8th Edition.
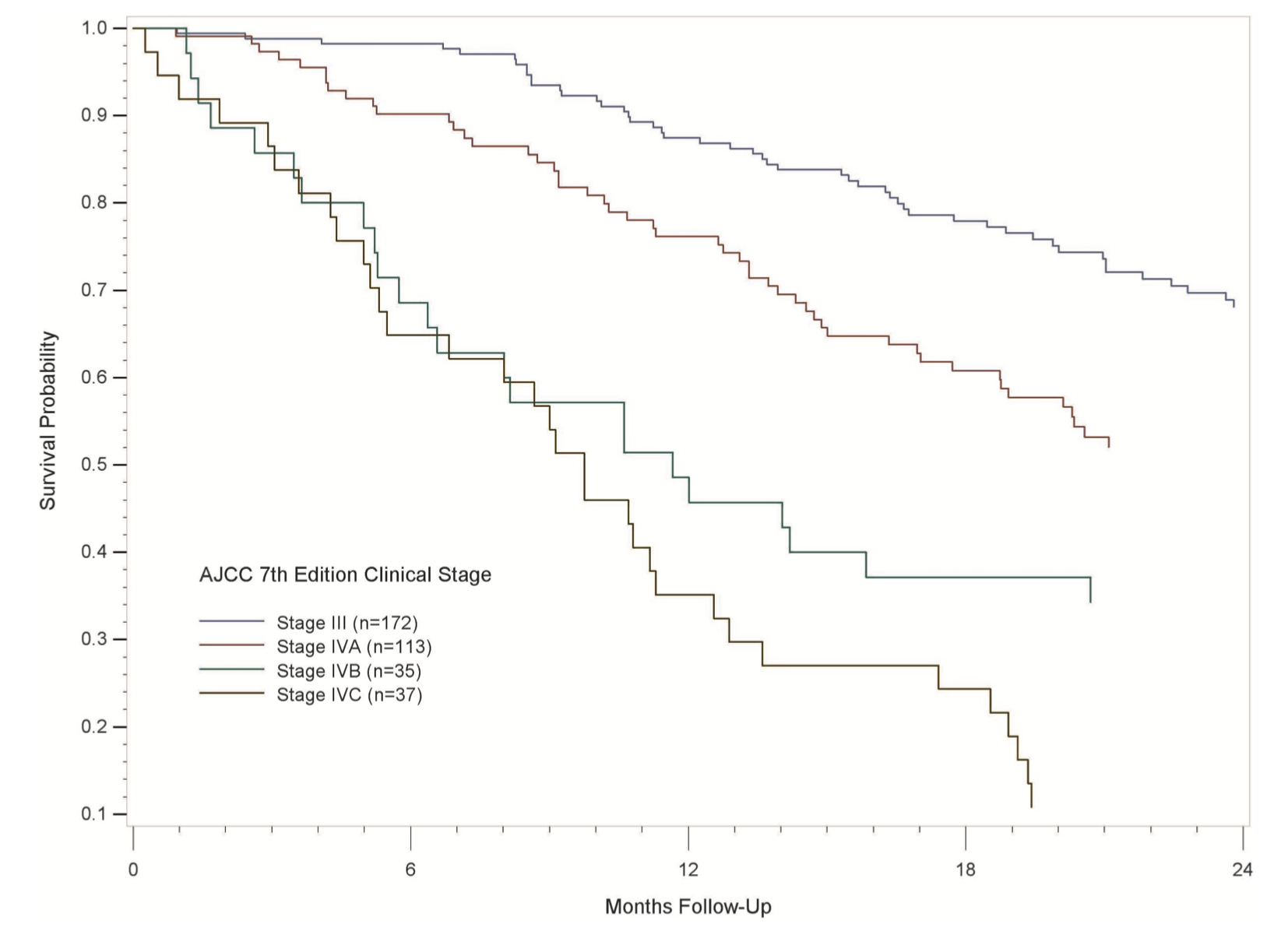
- Review of results with this new staging system showed good prognostic discrimination between stages and more recent studies (Luna-Ortiz et al) show superior prognostication versus the Ballantyne staging system.
Survival probability over time by stage (AJCC 7th Edition)
- Unchanged in the AJCC 8th Edition versus the 7th Edition.
- However the AJCC 8th Edition was later revised to exclude the dry vermillion lip and oral commissure from this staging system.
- In the initial version, the dry lip (ie. the vermillion) and oral commissure were considered both mucosal and part of the oral cavity.
- Melanomas involving the dry lip were staged as mucosal melanomas.
- Other carcinomas involving the dry lip were staged as oral cavity carcinomas.
- In the updated AJCC 8th Edition, the dry vermillion lip and oral commissure are no longer considered a mucosal surface and is now grouped with the cutaneous skin.
- As a result, dry lip melanoma is now staged as a cutaneous melanoma, and other dry lip carcinomas are now staged as cutaneous carcinomas of the head and neck.
| T Category |
Criteria |
| T3 |
- Limited to the mucosa and underlying soft tissue.
- No further subdivisions by thickness or dimensions.
|
| T4a |
- Tumour invasion into the deep soft tissue, cartilage, bone, or overlying skin.
|
| T4b |
- Tumour involvement of the brain, dura, skull base, lower cranial nerves (IX, X, XI, XII), masticator space, carotid artery, mediastinum, or pre-vertebral space.
|
General Rules
- There is no T1 or T2 category for mucosal melanoma; all primary tumours are classified as at least T3 due to the aggressive nature of the disease.
- Primary tumours limited to the mucosa and underlying soft tissue are considered T3.
- Locally advanced mucosal melanomas are classified as T4a and T4b.
- Mucosal melanoma in situ is very rare and is excluded from this staging system.
| N Category |
Criteria |
| NX |
Regional nodes cannot be assessed |
| N0 |
Regional lymph node metastasis absent |
| N1 |
Regional lymph node metastasis present |
| M Category |
Criteria |
| M0 |
No distant metastasis |
| M1 |
Distant metastasis present |
| III |
IVA |
IVC |
| IVA |
IVA |
IVC |
| IVB |
IVB |
IVC |
General Rules
- Only T3, N0 is classified as Stage III
- All T4b tumours are upstaged to Stage IVB (easy to remember).
- The presence of distant metastasis upstages to Stage IVC
- Stage IVA is used to classify T3/T4a tumours with regional LN metastasis, as well as T4a tumours without regional LN metastasis.







